This information will help you get ready for your HDR intracavitary brachytherapy (IN-truh-KA-vih-tayr-ee BRAY-kee-THAYR-uh-pee) for treatment of cervical or endometrial cancer at MSK.
Read through this resource at least once before your brachytherapy procedure and use it as a reference in the days leading up to your treatment. Bring it with you every time you come to MSK, including for your treatments. You and your healthcare team will refer to it throughout your care.
About the female reproductive system
Your reproductive system includes your ovaries, fallopian tubes, uterus, cervix, and vagina (see Figure 1).
Your uterus is located in your lower abdomen (belly) between your bladder and rectum (see Figure 2). The lower, narrow end of your uterus is called your cervix. Your cervix connects your uterus to your vagina, which leads to the outside of your body. Your ovaries and fallopian tubes are attached to the upper part of your uterus.
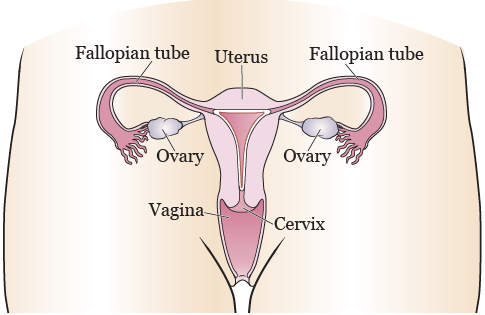
Figure 1. The female reproductive system (front view)
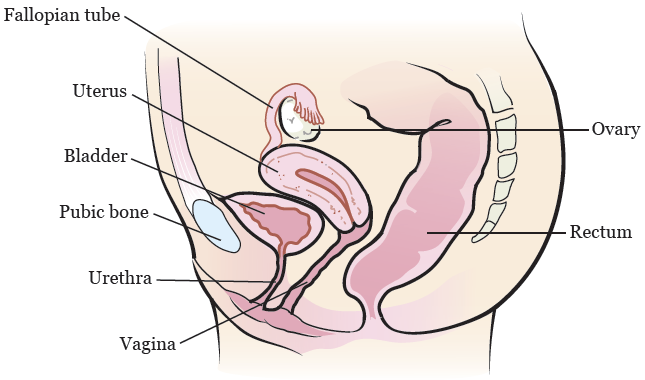
Figure 2. The female reproductive system (side view)
About HDR intracavitary brachytherapy
Brachytherapy is a type of radiation therapy. Radiation therapy kills cancer cells by making it hard for them to multiply.
With HDR brachytherapy, a radioactive source is placed inside or close to the tumor(s). This means that the tumor gets a large amount of radiation, while nearby healthy tissue gets less radiation and is less likely to be damaged. Iridium-192 is the radioactive source that will be used during your brachytherapy.
With HDR intracavitary brachytherapy, the radioactive source is placed into a cavity (open space) in your body, such as your uterus.
Most people have both HDR intracavitary brachytherapy and external beam radiation therapy.
What to expect
Before your first HDR intracavitary brachytherapy treatment, your healthcare provider will place an applicator into your uterus through your vagina. The applicator will hold the radioactive source during your treatments. The applicator itself isn’t radioactive, and you won’t be radioactive between treatments.
The applicator has 2 parts:
- Tandem: a thin metal tube with a closed end.
- Ring: a thin metal tube with a closed end that’s circular in shape.
The procedure to place the applicator will be done in the operating room while you’re asleep. For more information about the applicator placement and your first treatment, read the “During your procedure” section.
The applicator will stay in your uterus between your first and second treatments. You’ll stay in the hospital overnight while the applicator is in place. For more information about what to expect while you’re in the hospital, read the “In your hospital room” section.
Your second treatment will be the day after your first treatment. After your second treatment, the applicator will be removed and you’ll be able to leave the hospital. For more information about your second HDR brachytherapy treatment and applicator removal, read the “Your HDR intracavitary brachytherapy treatments” section.
The same procedure and treatment schedule will be repeated the following week for your third and fourth HDR brachytherapy treatments.
You’ll have a total of 2 applicator placements separated by 1 week. After each applicator placement, you’ll receive 1 HDR brachytherapy treatment right away and 1 HDR brachytherapy treatment on the next day. You’ll have a total of 4 HDR intracavitary brachytherapy treatments.
Your role on your radiation therapy team
You’ll have a team of healthcare providers working together to provide the right care for you. You’re part of that team, and your role includes:
- Arriving on time for your procedures.
- Asking questions and talking about your concerns.
- Telling someone on your radiation therapy team when you have side effects or if you’re in pain.
-
Caring for yourself at home.
- Quitting smoking, if you smoke. If you want to quit, call our Tobacco Treatment Program at 212-610-0507.
- Drinking liquids as instructed by your healthcare team.
- Eating the foods suggested by your healthcare team.
- Maintaining your weight.
Before your procedure
The information in this section will help you prepare for your procedure.
Read through this section when your procedure is scheduled and refer to it as your procedure date gets closer. It contains important information about what you need to do before your procedure. Write down any questions you have and be sure to ask your healthcare provider.
Getting ready for your procedure
You and your care team will work together to get ready for your procedure. Help us keep you safe by telling us if any of these things apply to you, even if you’re not sure.
-
I take an anticoagulant (blood thinner), such as:These are examples of medicines. There are others.
Be sure your healthcare provider knows all the medicines you’re taking.- Aspirin
- Heparin
- Warfarin (Jantoven®, Coumadin®)
- Clopidogrel (Plavix®)
- Enoxaparin (Lovenox®)
- Dabigatran (Pradaxa®)
- Apixaban (Eliquis®)
- Rivaroxaban (Xarelto®)
-
I take an SGLT2 inhibitor, such as:
- Canagliflozin (Invokana®)
- Dapagliflozin (Farxiga®)
- Empagliflozin (Jardiance®)
- Ertugliflozin (Steglatro®)
- I take prescription medicine(s), including patches and creams. A prescription medicine is one you can only get with a prescription from your healthcare provider.
- I take over-the-counter medicine(s), including patches and creams. An over-the-counter medicine is one you can buy without a prescription.
- I take dietary supplements, such as herbs, vitamins, minerals, or natural or home remedies.
- I have a pacemaker, automatic implantable cardioverter-defibrillator (AICD), or other heart device.
- I have sleep apnea.
- I have had a problem with anesthesia (A-nes-THEE-zhuh) in the past. Anesthesia is medicine to you sleep during a surgery or procedure.
- I’m allergic to certain medicines or materials, including latex.
- I’m not willing to receive a blood transfusion.
- I drink alcohol.
- I smoke or use an electronic smoking device, such as a vape pen or e-cigarette.
- I use recreational drugs, such as marijuana.
About drinking alcohol
It’s important to talk with your healthcare providers about how much alcohol you drink. This will help us plan your care.
If you drink alcohol regularly, you may be at risk for problems during and after your procedure. These include bleeding, infections, heart problems, and a longer hospital stay.
If you drink alcohol regularly and stop suddenly, it can cause seizures, delirium, and death. If we know you’re at risk for these problems, we can prescribe medications to help prevent them.
Here are things you can do before your procedure to keep from having problems.
- Be honest with your healthcare providers about how much alcohol you drink.
-
Try to stop drinking alcohol once your procedure is planned. Tell your healthcare provider right away if you:
- Get a headache.
- Feel nauseous (like you’re going to throw up).
- Feel more anxious (nervous or worried) than usual.
- Cannot sleep.
- Tell your healthcare provider if you cannot stop drinking.
- Ask your healthcare provider questions about drinking and procedures. All your medical information will be kept private, as always.
About smoking
If you smoke or use an electronic smoking device, you can have breathing problems when you have a procedure. Vapes and e-cigarettes are examples of electronic smoking devices. Stopping for even a few days before your procedure can help prevent breathing problems during and after your procedure.
Your healthcare provider will refer you to our Tobacco Treatment Program if you smoke. You can also reach the program by calling 212-610-0507.
About sleep apnea
Sleep apnea is a common breathing problem. If you have sleep apnea, you stop breathing for short lengths of time while you’re asleep. The most common type is obstructive sleep apnea (OSA). With OSA, your airway becomes fully blocked during sleep.
OSA can cause serious problems during and after a procedure. Tell us if you have or think you might have sleep apnea. If you use a breathing device, such as a CPAP machine, bring it on the day of your procedure.
Within 30 days of your procedure
Presurgical testing (PST)
You’ll have a PST appointment before your procedure. You’ll get a reminder from your healthcare provider’s office with the appointment date, time, and location. Visit www.msk.org/parking for parking information and directions to all MSK locations.
You can eat and take your usual medicines the day of your PST appointment.
It’s helpful to bring these things to your appointment:
- A list of all the medicines you’re taking, including prescription and over-the-counter medicines, patches, and creams.
- Results of any medical tests done outside of MSK in the past year, if you have them. Examples include results from a cardiac stress test, echocardiogram, or carotid doppler study.
- The names and telephone numbers of your healthcare providers.
You’ll meet with an advance practice provider (APP) during your PST appointment. They work closely with MSK’s anesthesiology (A-nes-THEE-zee-AH-loh-jee) staff. These are doctors with special training in using anesthesia during a procedure.
Your APP will review your medical and surgical history with you. You may have tests to plan your care, such as:
- An electrocardiogram (EKG) to check your heart rhythm.
- A chest X-ray.
- Blood tests.
Your APP may recommend you see other healthcare providers. They’ll also talk with you about which medicine(s) to take the morning of your procedure.
Fill out a Health Care Proxy form
If you have not already filled out a Health Care Proxy form, we recommend you do now. If you already filled one out or have any other advance directives, bring them to your next appointment.
A health care proxy is a legal document. It says who will speak for you if you cannot communicate for yourself. This person is called your health care agent.
- To learn about health care proxies and other advance directives, read Advance Care Planning for People With Cancer and Their Loved Ones.
- To learn about being a health care agent, read How to Be a Health Care Agent.
Talk with a member of your care team if you have questions about filling out a Health Care Proxy form.
7 days before your procedure
Follow your healthcare provider’s instructions for taking aspirin
Aspirin can cause bleeding. If you take aspirin or a medicine that has aspirin, you may need to change your dose or stop taking it 7 days before your procedure. Follow your healthcare provider’s instructions. Do not stop taking aspirin unless they tell you to.
To learn more, read How To Check if a Medicine or Supplement Has Aspirin, Other NSAIDs, Vitamin E, or Fish Oil.
Stop taking vitamin E, multivitamins, herbal remedies, and other dietary supplements
Vitamin E, multivitamins, herbal remedies, and other dietary supplements can cause bleeding. Stop taking them 7 days before your procedure. If your healthcare provider gives you other instructions, follow those instead.
To learn more, read Herbal Remedies and Cancer Treatment.
Ask about your diabetes medicines, if needed
You’ll need to stop eating and drinking the night before and morning of your procedure. If you take insulin or another medicine for diabetes, you may need to change the dose. Ask the healthcare provider who prescribes your diabetes medicine what you should do the morning of your procedure.
2 days before your procedure
Stop taking nonsteroidal anti-inflammatory drugs (NSAIDs)
NSAIDs, such as ibuprofen (Advil® and Motrin®) and naproxen (Aleve®), can cause bleeding. Stop taking them 2 days before your procedure. If your healthcare provider gives you other instructions, follow those instead.
To learn more, read How To Check if a Medicine or Supplement Has Aspirin, Other NSAIDs, Vitamin E, or Fish Oil.
1 day before your procedure
If you have any changes in your health or you need to cancel your procedure for any reason, call your radiation oncologist.
Note the time of your procedure
A staff member will call you after the day before your procedure. If your procedure is scheduled for a Monday, they’ll call you on the Friday before. If you do not get a call by , call 212-639-5014.
The staff member will tell you what time to arrive for your procedure. They’ll also remind you where to go.
This will be the following location:
Presurgical Center (PSC) on the 6th floor
Memorial Hospital
1275 York Avenue (between 67th and 68th Streets)
New York, NY 10065
B elevator to the 6th floor
Visit www.msk.org/parking for parking information and directions to all MSK locations.
The night before your procedure
The night before your procedure:
- Take the medicines your healthcare provider told you to take the night before your procedure. Take them with a small sip of water.
- Shower using soap and water the night before or the morning of your procedure.
Instructions for eating
Stop eating at midnight (12 a.m.) the night before your surgery. This includes hard candy and gum.
Your healthcare provider may have given you different instructions for when to stop eating. If so, follow their instructions. Some people need to fast (not eat) for longer before their surgery.
The morning of your procedure
Instructions for drinking
Between midnight (12 a.m.) and 2 hours before your arrival time, only drink the liquids on the list below. Do not eat or drink anything else. Stop drinking 2 hours before your arrival time.
- Water.
- Clear apple juice, clear grape juice, or clear cranberry juice.
- Gatorade or Powerade.
-
Black coffee or plain tea. It’s OK to add sugar. Do not add anything else.
- Do not add any amount of any type of milk or creamer. This includes plant-based milks and creamers.
- Do not add honey.
- Do not add flavored syrup.
If you have diabetes, pay attention to the amount of sugar in your drinks. It will be easier to control your blood sugar levels if you include sugar-free, low-sugar, or no added sugar versions of these drinks.
It’s helpful to stay hydrated before surgery, so drink if you are thirsty. Do not drink more than you need. You will get intravenous (IV) fluids during your surgery.
Stop drinking 2 hours before your arrival time. This includes water.
Your healthcare provider may have given you different instructions for when to stop drinking. If so, follow their instructions.
Take your medicines
If your healthcare provider told you to take certain medicines the morning of your procedure, take only those medicines with a sip of water. Depending on what medicines you take, this may be all, some, or none of your usual morning medicines.
If you take any medicine(s) for diabetes, remember that you might need to take a different dose than usual. Follow your healthcare provider’s instructions.
Things to remember
- Do not put on any lotion, cream, deodorant, makeup, powder, perfume, or cologne.
- Take off nail polish and nail wraps.
- Do not wear any metal objects. Take off all jewelry, including body piercings. The equipment used during your procedure can cause burns if it touches metal.
- Leave valuable items (such as credit cards, jewelry, or your checkbook) at home.
- If you wear contact lenses, wear your glasses instead. Wearing contact lenses during your procedure can damage your eyes.
What to bring
- A pair of loose-fitting pants, such as sweatpants.
- Your breathing device for sleep apnea (such as your CPAP), if you have one.
- Your Health Care Proxy form, if you have completed one.
- A case for your personal items (such as eyeglasses, hearing aid(s), dentures, prosthetic device(s), wig, or religious articles), if you have one.
- This guide. Your healthcare team will use this guide to teach you how to care for yourself after your procedure.
You may also want to bring the items below. You’ll be lying in bed most of the time you’re in the hospital. Having ways to pass the time will be helpful.
- Your cell phone and charger.
- Your portable music player.
- Things to read.
- Other electronic devices and chargers.
Once you’re in the hospital
You’ll be asked to say and spell your name and date of birth many times. This is for your safety. People with the same or a similar name may be having a procedure on the same day.
When it’s time to change for surgery, you’ll get a hospital gown, robe, and nonskid socks to wear.
Meet with a nurse
You’ll meet with a nurse before your procedure. Tell them the dose of any medications you took after midnight (12 a.m.) and the time you took them. Make sure to include prescription and over-the-counter medications, patches, and creams.
Your nurse may place an intravenous (IV) line in one of your veins, usually in your arm or hand. If your nurse does not place the IV, your anesthesiologist will do it in the procedure room.
Meet with an anesthesiologist
You will also meet with an anesthesiologist (A-nes-THEE-zee-AH-loh-jist). An anesthesiologist is a doctor with special training in anesthesia. They will give you anesthesia during your procedure. They will also:
- Review your medical history with you.
- Ask if you’ve had any problems with anesthesia in the past. This includes nausea (feeling like you’re going to throw up) or pain.
- Talk with you about your comfort and safety during your procedure.
- Talk with you about the kind of anesthesia you’ll get.
- Answer questions you have about anesthesia.
During your procedure
When it’s time for your procedure, you’ll either walk into the operating room or be taken in on a stretcher. A member of the operating room team will help you onto the operating bed. Compression boots will be placed on your lower legs. These gently inflate and deflate to help blood flow in your legs.
Once you’re comfortable, your anesthesiologist will give you anesthesia through your IV line and you’ll fall asleep. You’ll also get fluids through your IV line during and after your procedure.
After you’re fully asleep, a breathing tube will be placed through your mouth and into your windpipe to help you breathe. A urinary (Foley) catheter will also be placed to drain urine from your bladder.
Applicator placement
When they’re ready to start the procedure to place the applicator, your healthcare provider will gently dilate your cervix. They’ll place a small tube called a cervical stent into your cervix. Once the cervical stent is in place, the tandem will be placed into the stent. Then, the ring will be placed over the tandem, around your cervix.
The applicator will be held in place by 2 small balloons placed in your vagina and filled with water. The balloons will also push your bladder and rectum away from the applicator. This will help lower the amount of radiation they get during your treatments.
Once the applicator is in place, a magnetic resonance imaging (MRI) scan will be done to make sure it’s in a good position. Your healthcare provider will also use the scan to plan your treatment, including the dose (amount) of radiation that will be used. This will only take a couple of minutes. You’ll still be asleep.
HDR brachytherapy treatment
Once your treatment plan is ready, you’ll be brought to a separate treatment room. The position of the applicator will be checked again using x-ray images.
For your treatment, the applicator will be connected to a machine that holds the radiation source. The radiation source will travel from the machine into the applicator to deliver the treatment.
Once your treatment is complete, the source will move back into the machine and the applicator will be disconnected from the machine.
After your treatment, you’ll be brought to the Post-Anesthesia Recovery Unit (PACU).
After your procedure
The information in this section will tell you what to expect after your procedure, both during your hospital stay and after you leave the hospital. It will also tell you what to expect during your HDR brachytherapy treatments. Write down any questions you have and be sure to ask your healthcare provider .
In the Post-Anesthesia Care Unit (PACU)
When you wake up after your procedure, you’ll be in the Post Anesthesia Care Unit (PACU).
A nurse will be monitoring your body temperature, pulse, blood pressure, and oxygen levels. You’ll get oxygen through a thin tube that rests below your nose called a nasal cannula. You’ll have compression boots on your lower legs. You’ll also have a Foley catheter in your bladder to monitor the amount of urine you’re making.
You may have some pain after your procedure. Your healthcare providers will ask you about your pain often. You’ll have a pain pump called a patient-controlled analgesia (PCA) device. PCA uses a computerized pump to deliver pain medicine into your IV line. To learn more, read Patient-Controlled Analgesia (PCA). If your pain isn’t relieved, tell one of your healthcare providers.
There isn’t anything radioactive in your body between your treatments. After your stay in the PACU, you’ll be taken to your hospital room.
In your hospital room
While the applicator is in place, you’ll need to lie still on your back in bed. You must stay in bed until the applicator is removed. You’ll be able to raise the head of your bed a little bit, about 20 degrees. You won’t be able to move your hips or legs, but you can wiggle your toes. You’ll have compression boots on your legs to help prevent blood clots and improve blood flow. You’ll be able to move your arms and upper body.
We understand that lying still and flat in bed can be challenging. You’ll be able to read and use your phone and other electronic devices.
If you need help while you’re in your room, use your call bell to let a nurse know. The call bell is by the side of your bed. Your nurse will show you how to use the call bell system.
Your nurse will give you an incentive spirometer and teach you how to use it. They’ll ask you to do deep breathing exercises using your incentive spirometer. This helps your lungs expand, which prevents pneumonia. To learn more, read How To Use Your Incentive Spirometer.
You’ll follow a low-residue diet while you’re in the hospital. A low-residue diet has low amounts of fiber, which will help you have fewer bowel movements. You’ll also get medicine to keep you from having a bowel movement. You may want to avoid eating foods that cause gas or make you feel bloated. You’ll eat all of your meals in bed.
The Foley catheter will stay in your bladder until your applicator is removed.
Your HDR intracavitary brachytherapy treatments
For your HDR brachytherapy treatments, your bed will be moved from your room to the Brachytherapy Suite in the Department of Radiation Oncology. You’ll talk with your healthcare provider before or after your treatment.
In the Brachytherapy Suite, your radiation therapist will check the position of the applicator using x-ray images. Once they know the applicator is in a good position, your radiation therapist will connect the applicator to the machine that holds the radiation source.
Once everything is ready, your radiation therapist will leave the room while you receive your treatment. The room has a video camera, microphone, and speaker so your radiation therapist can see, hear, and talk to you at all times.
During your treatment, the radiation source will move from the machine into the applicator. You won’t feel any pain or discomfort during your treatment. You won’t see or feel the radiation. You may hear a clicking sound from the machine.
Your treatment will take about 10 to 20 minutes.
After your treatment is done, the radiation source will move back into the machine. Your radiation therapist will come into the room and disconnect the applicator from the machine.
Applicator removal
Right after your second and fourth treatments (the treatments you’re awake for), your nurse will give you medicine to make you relaxed and sleepy. Once you’re relaxed, the applicator and Foley catheter will be removed and you’ll be brought back to your hospital room.
After the applicator is removed, you may feel some cramping in your uterus and pressure in your vaginal area. These feelings usually go away over a couple of hours. Ask your nurse for pain medicine if you’re uncomfortable.
You’ll be discharged from the hospital the same day.
At home
After your treatments, you aren’t radioactive and don’t need to follow any radiation precautions.
You can go back to moving around and eating normally as soon as you leave the hospital.
You may have cramping for a day after your treatment. You can take an over-the-counter pain reliever such as ibuprofen (Advil® or Motrin®) or acetaminophen (Tylenol®) as needed. Do not take aspirin, products that contain aspirin, or vitamin E for at least 1 week after your procedure. Your healthcare provider will tell you when it’s safe to start talking them again.
Follow the guidelines below after you leave the hospital.
- Walk around and do light activities on the days following your treatment.
- Do not lift anything heavier than 10 pounds (4.5 kilograms) for 6 weeks following your treatment.
- You can shower after you’re discharged from the hospital, but do not take baths or swim in a pool for 6 weeks following your treatment.
- You can drive as long as you aren’t taking any prescription pain medicines that make you sleepy.
-
Do not put anything inside your vagina (such as tampons and douches) or have vaginal intercourse for 6 weeks following your treatment.
- Your care team may tell you to start vaginal dilator therapy 2 to 3 weeks after your treatment. If they do, it’s OK to put the dilators in your vagina. Do not put anything else inside your vagina.
Side effects of HDR intracavity brachytherapy
You may have side effects after your treatment. Talk to your healthcare provider if you have questions about side effects.
Vaginal scarring and loss of elasticity
After HDR brachytherapy, your body will start to heal. Your vaginal walls may start to stick together from scar tissue. Your vaginal tissue may also become less elastic. These changes can cause pain and discomfort and make things such as vaginal exams and vaginal intercourse more difficult.
Using a vaginal dilator can help keep scar tissue from forming. It also helps your vaginal tissue stay elastic. Vaginal dilator therapy is a form of physical therapy you can use throughout your life. It’s very important for you to use vaginal dilator therapy after treatment. It will:
- Allow your healthcare provider to do a more thorough vaginal exam.
- Make vaginal exams more comfortable for you.
- Keep your vagina from becoming too narrow.
- Keep your vagina more elastic.
- Allow you to have vaginal sex with less discomfort.
Your nurse will give you a vaginal dilator kit and explain how and when to use it. To learn more, read How To Use a Vaginal Dilator.
Vaginal bleeding
You may have mild vaginal bleeding (spotting) after going home. If you have heavy vaginal bleeding (bleeding that requires more than 3 pads per day), call your healthcare provider.
Use sanitary pads for vaginal bleeding. Do not use tampons.
Vaginal dryness
You may have vaginal dryness after your treatment. The dryness may last for the rest of your life. To help, you can use a vaginal moisturizer.
Vaginal moisturizers help to increase moisture in your vagina and improve tissue quality. They can be used up to 3 to 5 times a week. You can use them at any time, not only before or during sexual activity.
Over-the-counter vaginal moisturizers don’t have any hormones. You can buy them online or at your local pharmacy without a prescription. See below for information about types of vaginal moisturizers and how to use them.
Hydrating moisturizers
-
HYALO GYN®
- This moisturizer can be applied both inside of your vagina and on your vulva.
- You can buy HYALO GYN online at www.hyalogyn.com.
-
Replens™ Long-Lasting Vaginal Moisturizer
- This vaginal moisturizer can be inserted into your vagina with a disposable applicator or applied to your vulva.
- You can buy Replens Long-Lasting Vaginal Moisturizer at your local pharmacy.
Soothing (natural oil) moisturizers
-
Carlson® Key–E® Suppositories
- These are suppositories (solid medicines that dissolve) that you insert into your vagina with a disposable applicator. They work best if you use them at bedtime.
- You can buy Carlson Key-E suppositories online at www.carlsonlabs.com
- Natural oils, such as vitamin E or coconut oil
If you need more help or support, contact the Female Sexual Medicine and Women’s Health Program at 646-888-5076.
Vaginal or anal irritation
Your vaginal or anal area may become irritated after your treatment. Avoid rubbing the area, because it can lead to more irritation.
To help with irritation:
- Use a warm, wet cloth to cleanse the area.
- Use a sitz bath. A sitz bath is a warm, shallow bath that cleanses your perineum (the area between your vulva and anus). You can buy a plastic sitz bath that fits over your toilet at your local pharmacy. Don’t take a regular bath for 6 weeks after your treatment.
- Use a peri-bottle (small plastic bottle with a squirt tip) to wash your vaginal area, anal area, or both with warm water. You can buy a peri-bottle at your local pharmacy.
When to call your healthcare provider
Call your healthcare provider if you have:
- A fever of 100.4 °F (38 °C) or higher.
- Chills.
- Vaginal bleeding requiring more than 3 pads per day.
- Cloudy or foul smelling urine.
- Blood in your urine.
- Watery bowel movements (diarrhea) more than 3 times in 1 day that isn’t helped by medicine.
- No bowel movements in 3 days.
- Bleeding from your rectum.
- Nausea or vomiting that keeps you from eating or drinking.
- Pain in your abdomen or pelvis that isn’t helped by medicine.
- Shortness of breath (difficulty breathing) that’s new or getting worse.
- A faster heartbeat than usual.
- A cough that’s new or getting worse.
- Leg pain or cramping that’s new or getting worse.
- Swelling in one or both legs, calves, ankles, or feet that’s new or getting worse.