This information explains why it’s important to control your blood glucose (blood sugar) during cancer treatment at MSK. It also has information about the basic skills you’ll need to manage your blood glucose at home. Controlling your blood glucose will help you feel better and help prevent problems during treatment.
About hyperglycemia during cancer treatment
You’re getting this booklet because you have hyperglycemia (high blood sugar) and are getting cancer treatment. Hyperglycemia (HY-per-gly-SEE-mee-uh) means you have more glucose (sugar) than normal in your blood.
You may have diabetes, or short-term hyperglycemia. Short-term hyperglycemia may be related to your treatment plan and is common. About 3 out of every 10 of people with cancer will have hyperglycemia during treatment.
Hyperglycemia during cancer treatment can raise your risk of:
- Infection
- Poor healing after surgery
- Fatigue (feeling more tired than usual)
- Neuropathy (tingling or losing feeling in your fingers and toes)
- Pain
- Long-term problems related to diabetes
During cancer treatment, it’s important to manage chronic health conditions such as diabetes, high blood pressure, and high cholesterol. These can cause long-term health problems even after you finish treatment.
For some treatments, your blood sugar must be within a target range. A target range is when your glucose is not too high or too low.
We may need to stop your treatment if your blood glucose goes very high and stays high. This depends on the type of treatment you’re getting. Your healthcare provider will give you more information.
Diet and physical activity are the best ways to manage blood glucose levels. You may also need medicine. Your diabetes healthcare provider will work with you on a plan to manage your blood sugar at home.
During treatment, it’s common to have less energy and a poor appetite (not feeling hungry). This can make it harder to manage your blood glucose levels with diet and activity. We’re here to support and help you.
What are diabetes survival skills?
There’s a lot of information to learn about diabetes. This resource provides basic information, also called diabetes survival skills, to start safely managing your blood glucose at home.
Your outpatient diabetes healthcare provider will follow-up and teach you more about these skills after discharge (leaving the hospital).
This resource has information about:
- Blood glucose monitoring
- Hyperglycemia
- Hypoglycemia
-
Understanding your diabetes medicine
- Insulin
- Oral medicine
- Non-insulin injectable medicine
- Nutrition
- Follow-up care
Common questions about diabetes
I have a lot going on with my cancer treatment and feel like I cannot handle it all. Is it OK to wait to start diabetes treatment?
It’s important to start diabetes treatment as soon as your diabetes healthcare provider prescribes it. Controlling your blood glucose can help you feel better and make it easier to get through treatment. It helps lower the risk of infection and other health problems caused by hyperglycemia, such as dehydration.
How can I prevent other health issues caused by diabetes?
There is no cure for diabetes. Keeping your body at a healthy weight can help it use insulin more easily. It also helps your body manage your blood glucose levels.
Controlling your blood glucose levels is the best way to prevent other health issues caused by diabetes. You can do this by taking your diabetes medicine as prescribed.
Knowing your blood glucose level is the first step to preventing hyperglycemia. Check your blood glucose regularly. Read About Hyperglycemia (High Blood Sugar) to learn more.
Keep a healthy lifestyle through diet and exercise. To learn more about eating a healthy diet, call 212-639-7312 to talk with a clinical dietitian-nutritionist.
Common terms about diabetes care
Blood glucose (BG) levels: Also called blood sugar (BS) or glucose levels. This is measured by fingerstick.
Blood glucose (BG) log: Used to track blood glucose over time.
Blood glucose meter (BGM): Also called BG meter, glucometer, or glucose machine. This is used to do a fingerstick blood glucose check.
Carbohydrates: Your body’s main source of glucose. These are also called carbs.
Continuous glucose monitor (CGM): A small device you place on your arm or stomach that reads your glucose levels every few minutes.
Endocrinologist (EN-doh-krih-NAH-loh-jist): A doctor with special training in endocrine problems, such as diabetes.
Glucose: The body’s main source of energy. Your body stores extra glucose in your muscles and liver for energy. It also stores extra glucose as fat.
Hemoglobin (HEE-moh-GLOH-bin) A1c (HbA1c): The measure of your average blood sugar level over the past 3 months.
Hour of sleep (HS): At bedtime, usually a set time of night before you go to bed.
Insulin: A hormone that moves glucose from the blood to the body’s cells. Insulin is also a medicine you can inject if your body does not make enough insulin on its own.
Insulin sliding scale: A scale healthcare providers use to decide how much insulin you need to take. This scale often is part of a blood glucose log.
Macronutrients: Major food groups, such as carbohydrates, protein, and fat.
NPO: Nothing by mouth. Instructions for when to stop eating and drinking.
Polydipsia (pah-lee-DIP-see-uh): Extreme thirst.
Polyuria (pah-lee-YOOR-ee-uh): Urinating (peeing) often.
Post-prandial: After a meal.
Pre-prandial: Before a meal.
Target range: When your blood glucose is not too high or too low.
Titration (tih-TRAY-shun): Adjusting your medicine over time by tapering (lowering) or escalating (raising) the dosage.
How to Check Your Blood Sugar Using a Blood Glucose Meter
This information describes how to check your blood glucose level using a blood glucose meter.
The steps in this resource are specific to the Contour® Next One blood glucose meter and Microlet® Next lancing device. If you’re using a different type of blood glucose meter or lancing device, follow the instructions that came with it. All blood glucose meters and lancing devices are slightly different.
About the Microlet Next lancing device
Your lancing device holds the lancet (needle) you’ll use to prick your finger. It has 6 main parts (see Figure 1).
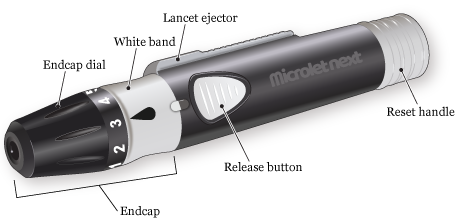
- The endcap covers the lancet until you’re ready to use it.
- The endcap dial controls how deeply the lancet will prick your finger.
- The white band connects the endcap to the rest of the lancing device. The endcap is locked onto the lancing device when the black drop is in line with the release button.
- The release button makes the tip of the lancet spring out to prick your finger.
- The reset handle resets the lancet if you need to prick your finger again.
- The lancet ejector pushes the lancet out of the lancing device once you’re done using it.
Your Microlet Next lancing device works with Microlet lancets. Microlet Next lancets come in different colors, but there’s no difference between them.
About your Contour Next One blood glucose meter
A blood glucose meter measures the amount of sugar in your blood. It has 3 main parts (see Figure 2).
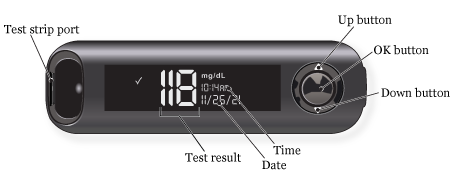
- The test strip port is where you’ll put the blood glucose test strip into the meter. Your Contour Next One glucose meter will only work with Contour Next test strips.
- The screen shows information such as the meter’s status, your blood glucose level, and the date and time.
-
The buttons are how you control the meter.
- To scroll up, press the up button. Hold it to keep scrolling.
- To scroll down, press the down button. Hold it to keep scrolling.
- To accept a selection, press the OK button.
- To turn your meter on or off, press and hold the OK button.
You need to set up your meter before using it for the first time.
You do this by:
- Accepting the blood glucose target range of 70-180 milligrams per deciliter (mg/dL).
- Setting the time.
- Setting the date.
Your meter will not work until you set it up.
Watch Contour® Next One Video: Doing Your First Test for instructions on how to set up your meter.
Do not put your glucose meter under water. If you notice it’s dirty, wipe it with a damp cloth or alcohol pad.
The Contour Diabetes app
The Contour Diabetes app works with your Contour Next One blood glucose meter. It lets you make notes, set reminders, see your results in a graph, and share your reports. If you want to use the app, you can download it from the Apple App Store® or Google Play™ store.
You do not need to download the Contour Diabetes app if you do not want to. The Contour Next One blood glucose meter works without the app.
The Contour Next One user guide
To learn more about the Contour Next One blood glucose meter and Contour Diabetes app, read the Contour Next One user guide. You can read the copy that came with your meter or find it at www.contournextone.com/getting-started.
Instructions for checking your blood sugar
Your healthcare provider will tell you how often to check your blood glucose. They’ll also tell you what your blood glucose level should be. This is called your blood glucose target range. Your blood glucose target range is based on your overall health and current treatment plan.
When you’re ready to start, wash your hands with soap and water. Dry them very well. Touching a blood glucose test strip with damp hands can damage it or make your result less accurate.
Gather your supplies
Set up your supplies on a clean surface. It’s helpful to arrange them in the order you’ll use them (see Figure 3).

You’ll need:
- Your lancing device.
- A new lancet.
- Your blood glucose meter.
- Your blood glucose test strips.
- An alcohol pad (if you do not have access to a sink to wash your hands).
- A dry tissue or gauze pad (if you do not have access to a sink to wash your hands).
- Your blood glucose log.
- A trash can.
- A solid container to throw away the used lancet, such as a heavy plastic laundry detergent bottle with a lid. Read How to Store and Get Rid of Your Home Medical Sharps for more information about choosing a container.
When you take a blood glucose test strip out of the container, set it on top of your meter. This helps keep it clean and dry and makes it easier to pick up. Make sure to close the glucose test strip container tightly. Humidity from the air can damage the strips.
Get your lancing device ready
-
Twist the white band on your lancing device to the right to unlock the endcap (see Figure 4).
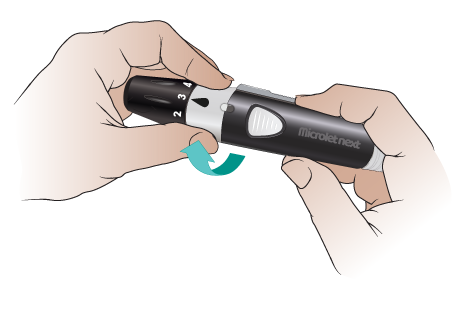
Figure 4. Twist the white band to the right - Pull the endcap straight off (see Figure 5).

- Carefully twist the round tab 3 times. Be careful not to bend it. Pull the tab off and set it aside to use later (see Figure 6). You should see a small needle where the tab was.

- Put the endcap back on your lancing device in the unlocked position (see Figure 7).

-
Twist the white band to the left to lock the endcap on (see Figure 8).

Figure 8. Twist the white band to the left -
Turn the black part of the endcap dial to set the puncture depth (see Figure 9). It’s best to start with level 1 or 2. You can set it to a higher level if you do not get a big enough blood drop.

Figure 9. Set the puncture depth
Your lancing device is now ready. Set it down. Pick up your blood glucose meter and test strip.
Get your blood glucose meter ready
- Hold the test strip with the printed side facing you.
- Hold your blood glucose meter with the screen and buttons facing you.
-
Put the grey square end of the test strip into your meter’s test strip port (see Figure 10).

Figure 10. Put the test strip into the port
Your meter should beep and turn on after you put the test strip in the port. If it does not:
- Make sure you pushed the test strip all the way into the port.
- Make sure the end of the test strip with the grey square is in the port.
- Make sure the printed side of the test strip is facing you.
Your blood glucose meter is now ready. It will stay on for 3 minutes after you put in the test strip. If you do not apply a drop of blood to the tip of the test strip in that time, it will beep and turn off. If this happens, pull the test strip out and put it back into the port.
Do not apply blood to the test strip before you put it into the meter or when the meter is off. If you do, that strip will be ruined. You’ll have to start over with a new one.
Prick your finger
-
Choose which finger you’re going to prick. We recommend using the side of your fingertip (see Figure 11). The middle and top of your fingertip are more sensitive.
- Use a different spot each time. This will help prevent sore spots. Remember that you can use both sides of each fingertip.
- If you have not already washed your hands, clean the area with the alcohol pad. Dry it with the clean tissue or gauze pad.

Figure 11. Hold the lancing device firmly against the side of your finger -
Hold your lancing device firmly against the side of your finger (see Figure 12) and press the release button. Then move the lancing device away from your finger right away. Look for a blood drop.You may need to gently massage or squeeze your finger (see Figure 12). Do not do this too hard. If you do, your results may not be accurate.If the blood drop is too small, you’ll need to prick your finger again. It’s OK to use the same lancet.

Figure 12. Gently squeeze your finger to get a blood drop
a. Pull the white reset handle on your lancing device until you hear it click into place (see Figure 13).

b. Turn the endcap dial to increase the puncture depth by 1 level.
c. Make sure you have the lancing device pressed firmly against the side of your finger.
d. Press the release button. Then move your lancing device away from your finger right away.
e. Look for a blood drop. You may need to massage your finger gently. If the blood drop is bigger than you needed, lower the puncture depth by 1 next time you use your lancing device. This means the lancet will not prick your finger as deeply.
Touch the blood glucose test strip to the blood drop
-
Once you have a big enough blood drop, touch the tip of the test strip to the drop (see Figure 14). The blood will be drawn into the test strip. Putting the blood on the top, bottom, or side of the strip will not work.
- If there is not enough blood on the first try, your meter will beep twice, and a blood drop will flash on the display. You can apply more blood to the test strip within 60 seconds.
- If you do not apply enough blood within 60 seconds, your meter will show an error code. If this happens, pull out the test strip and throw it away. Start again with a new test strip. Increase the puncture depth on your lancing device, if needed.

Figure 14. Touch the end of the test strip -
When you’ve applied enough blood to the test strip, your meter will beep and count down from 5. Your blood glucose level will appear on the screen and you’ll see a color near the test strip port. This is called the Target Light or smartLIGHT. You’ll see green if your result is in the target range, yellow if it’s too high, or red if it’s too low.
- When you first get your Contour Next One blood glucose meter, the target blood glucose range will be 70 to 180 mg/dL.
- If your diabetes provider gives you a different target range, you can change it using the Contour Diabetes app.
- If you do not want to use the smartLIGHT feature, you can turn it off using the Contour Diabetes app.
Write down your blood sugar level
Write your blood glucose level in your blood glucose log. Your result will stay on the screen until you take out the test strip or for 3 minutes.
Make sure your blood glucose meter is right-side up when you read it. To quickly check, make sure you can read the time and date.
Throw away the test strip and used lancet
-
Firmly pull the test strip out of your blood glucose meter (see Figure 15). Throw it away in the trash can. It’s OK to put it with your regular trash.

Figure 15. Pull the test strip out of your blood glucose meter - Twist the white band on your lancing device to the right to unlock the endcap. Pull the endcap straight off.
-
Put the round plastic tab you removed from the top of the lancet earlier on a flat surface. Push the end of the lancet firmly into the plastic tab (see Figure 16). The tab will cover the lancet so you will not accidentally prick yourself.

Figure 16. Push the end of the lancet into the plastic tab -
Hold the lancet over your plastic sharps container. Slide the lancet ejector forward until the lancet falls into the plastic sharps container (see Figure 17).
- Do not pull the lancet out with your fingers. The plastic tab can easily come off. If it does, you may prick yourself with the needle.

Figure 17. Eject the lancet into the sharps container - Slide the lancet ejector back into place. Put the endcap back on your lancing device. Twist the white band to the left to lock on the endcap.
Keeping track of your results
- Your healthcare provider will tell you how to keep track of your blood glucose levels and medicine doses. Follow their instructions.
- Bring your blood glucose log to all your appointments. This information will help your healthcare provider decide if they should change your current treatment plan. If you have questions about checking your blood glucose, ask your healthcare provider.
Where to buy supplies
Talk with your diabetes healthcare provider to get a refill prescription for blood glucose test strips and lancets. You must get refills from your local pharmacy. MSK’s outpatient pharmacy does not carry these supplies.
If your blood glucose meter is battery-powered, make sure to always have extra batteries. The Contour Next One blood glucose meter uses 2 CR-2032 batteries. You can buy these batteries online or at your local electronics store, hardware store, or supermarket.
Contour Next One Video - Doing your first test
About Hyperglycemia (High Blood Sugar)
This information describes hyperglycemia (HY-per-gly-SEE-mee-uh), what causes it, and how to recognize, prevent and treat it. It also talks about different types of diabetes.
What is hyperglycemia?
Hyperglycemia is when too much glucose (sugar) builds up in your bloodstream. This can cause you to feel tired and run down or get sick.
There are 2 types of hyperglycemia:
- Acute hyperglycemia happens when a person’s blood glucose spikes suddenly over a period of days or weeks.
- Chronic hyperglycemia happens when a person’s blood glucose rises slowly over a long period of time.
Causes of hyperglycemia
Hyperglycemia can happen if your body doesn’t make enough insulin or can’t easily use the insulin it makes. Insulin is a hormone that lets glucose go from your bloodstream into your cells. If your body does not have enough insulin, glucose stays in your bloodstream and causes hyperglycemia.
Treatment-related hyperglycemia
Some cancer treatments can raise your blood glucose and cause hyperglycemia, including chemotherapy and steroid treatment. Getting nutrition from tube feedings or total parenteral nutrition (TPN) can also cause hyperglycemia.
You may need to keep your blood glucose within a certain range during certain treatments. Your diabetes healthcare provider may prescribe insulin or oral (by mouth) diabetes medicine to improve your glucose levels. They will also explain how to check your blood sugar and how often.
Treatment-related hyperglycemia usually goes away after treatment ends. If it doesn’t, you may have had blood glucose issues before treatment. Keep checking your blood glucose and taking your medicine until your diabetes healthcare provider tells you to stop.
Risk factors for hyperglycemia
Hyperglycemia is more likely to happen if you:
- Have type 1 or type 2 diabetes mellitus (DM) or pre-DM.
- Are not getting enough diabetes medicine to control your blood glucose levels.
- Are not injecting insulin correctly.
- Are using expired insulin or insulin that has gone bad. This can happen if insulin gets too hot or too cold.
- Have not been active enough.
- Eat too many carbohydrates. Read How To Manage Your Blood Glucose (Blood Sugar) With Your Diet to learn more.
- Are getting nutrition from tube feedings or TPN.
- Are sick or have an infection.
- Have physical stress, such as an injury or surgery.
- Have emotional stress, such as from treatment or problems in your personal life.
- Have had all or part of your pancreas removed.
-
Are taking certain medications. Examples include:
- Steroids, such as prednisone or dexamethasone (Decadron®).
- Immunosuppressants, such as tacrolimus and sirolimus.
- Certain types of chemotherapy, targeted therapy, immunotherapy, or hormone therapy. Talk with your healthcare provider to learn more.
Signs and symptoms of hyperglycemia
Your body’s cells need glucose for energy to work as they’re supposed to. For example, if the cells in your muscles don’t have energy, you may feel tired and run down. If your white blood cells don’t have energy, your body can struggle to fight off infection.
The signs and symptoms of high blood sugar can vary from mild to severe (very bad). They may happen acutely (suddenly) if there is a specific trigger. These include developing type-1 diabetes mellitus (T1DM) or steroid-induced hyperglycemia (high blood sugar caused by steroids).
For people with type-2 diabetes mellitus (T2DM), symptoms usually start out mildly and develop slowly over a long time. Mild signs and symptoms can be hard to recognize and may not feel the same to everyone. Because of this, it can take many years to notice or diagnose T2DM.
Acute hyperglycemia
Acute hyperglycemia happens suddenly. Signs and symptoms of acute hyperglycemia include:
- Feeling very thirsty.
- Having a dry mouth.
- Feeling like you need to urinate (pee) often.
- Having dry skin.
- Feeling more hungry than usual.
- Having blurry vision.
- Feeling drowsy.
Severe hyperglycemia
Acute hyperglycemia can get worse if it is not treated. This can lead to a diabetes emergency, such as diabetic ketoacidosis (DKA).
DKA can be life-threatening. If you have DKA or think you have DKA, seek medical attention right away. Call your diabetes healthcare provider, go to your local emergency room, or call 911. Read Diabetic Ketoacidosis (DKA) and Ketone Urine Testing to learn more.
Signs and symptoms of DKA include:
- Feeling confused.
- Feeling shortness of breath.
- Having a dry mouth.
- Feeling weak.
- Having abdominal (belly) pain.
- Feeling nauseous (like you’re going to throw up) or vomiting (throwing up).
- Falling into a coma.
Chronic (long-term) hyperglycemia
Chronic hyperglycemia develops over a long time. Signs and symptoms of chronic hyperglycemia include:
- Having wounds that heal more slowly than usual.
- Getting worse infections or infections more often than usual.
- Having little to no energy.
- Neuropathy (tingling or losing feeling in your fingers and toes).
- Skin changes, such as acanthosis nigricans (AK-un-THOH-sis NI-gruh-KANZ). These are dark, thick areas of soft skin. They usually form on the back of the neck, armpits, or groin area.
- Gum disease. Signs of this include red, sore, irritated gums.
- Any or all of the signs and symptoms of acute hyperglycemia.
How to prevent hyperglycemia
Check your blood glucose
Knowing your blood glucose level is the first step to preventing hyperglycemia. Checking your blood glucose tells you if your glucose levels within your target range. The target range is when your glucose is not too high or too low.
Your diabetes healthcare provider or educator will:
- Tell you how often to check your blood glucose.
- Set your target range based on your health and treatment plan.
- Use your blood glucose readings to adjust your medications as needed.
What is a safe blood glucose range?
MSK’s target blood glucose range for people getting cancer care is usually 100 to 200 milligrams per deciliter (mg/dL). Your diabetes healthcare provider may have different recommendations for you.
How to check your blood glucose at home
You can check your blood glucose level at home using one of these devices:
- A blood glucose meter (or glucometer). You can buy a blood glucose meter at your local pharmacy with or without a prescription. Read How to Check Your Blood Glucose (Blood Sugar) Using a Blood Glucose Meter to learn more.
- A continuous glucose monitor (CGM). Read About Your Continuous Glucose Monitor (CGM) to learn more.
Keep track of your blood glucose results and medicine
Keep track of your blood glucose results and doses of insulin on a blood glucose log. This will help your diabetes healthcare provider safely adjust your medications.
Practice a healthy and active lifestyle
The best way to prevent hyperglycemia and manage your blood glucose is to practice a healthy and active lifestyle. Use your blood glucose readings to guide lifestyle choices to reach your target range. Talk with your diabetes healthcare team about how to do this safely.
Here are some tips for managing your blood glucose levels at home:
Follow a healthy diet
Follow a healthy diet and stay on your meal plan. We recommend following a consistent carbohydrate meal plan, which means having a certain amount of carbohydrates for each meal. Read How To Manage Your Blood Glucose (Blood Sugar) With Your Diet to learn more.
Stay well-hydrated
Drink enough liquids to stay hydrated. Follow your healthcare provider’s instructions for how much liquid to drink.
Drink sugar-free liquids
Drink sugar-free, flavored water, sparkling water (seltzer) or other zero-calorie drinks. Avoid regular soda and fruit juice made with real fruit. These usually have a lot of sugar and can raise your blood glucose.
Get enough physical activity
Physical activity can help keep your blood glucose at a healthy level. Follow your healthcare provider’s instructions on how much activity is safe for you.
Take your diabetes medicine as prescribed
Follow your diabetes healthcare provider’s instructions for taking your diabetes medicine. They will help you plan for what to do if you miss a dose of your medicine.
When to call your diabetes healthcare provider
MSK recommends talking with your diabetes healthcare provider within 10 days after leaving the hospital. Call them if:
- You have new hyperglycemia.
- You were just diagnosed with diabetes.
- Your diabetes medicines have changed.
- Your blood glucose has been above your target range most of the time over the past 2 to 3 days.
- Your blood glucose is lower than 70 mg/dL or higher than 400 mg/dL. These can be dangerous.
- You’re vomiting, or you have diarrhea more than 3 times in 24 hours (1 day).
- You have DKA or think you have DKA.
- You do not feel well and are unsure if you should take your diabetes medications.
- You have a fever of 101° F (38.3° C) or higher.
Go to your local emergency room or call 911 if you cannot contact your healthcare provider right away.
About Hypoglycemia (Low Blood Sugar)
This information explains what hypoglycemia (HY-poh-gly-SEE-mee-uh) is and what signs to look for. It explains how to treat it and how to prevent it from happening.
What is hypoglycemia?
Hypoglycemia is when your blood glucose (blood sugar) level goes too low. This usually happens when your blood glucose goes below 70 milligrams per deciliter (mg/dL).
Your body uses glucose as its main source of energy. If there isn’t enough glucose in your bloodstream, you may have trouble thinking clearly and doing your usual tasks safely. This can happen if you have not eaten enough or are more active than usual.
It is important to treat hypoglycemia right away. If you take medication for diabetes, your healthcare provider may need to change the dosage. Contact the provider who prescribes your diabetes medication any time you have hypoglycemia.
Signs of hypoglycemia and what to look for
Some people show different warning signs when their blood glucose is low. Others may show no signs at all.
Warning signs of hypoglycemia include:

Check for hypoglycemia by measuring your blood glucose at home. Read How to Check Your Blood Glucose (Blood Sugar) Using a Blood Glucose Meter for more information. You can also watch How To Check Your Blood Glucose (Blood Sugar) Using a Blood Glucose Meter.
How to treat hypoglycemia
Follow the rule of 15/15 if your blood sugar is below 70 mg/dL and you’re awake and alert.
Rule of 15/15
- Have 15 grams of sugar. If your blood sugar is below 70 mg/dL, have a simple, rapid-acting sugar. These are foods and drinks that have glucose, dextrose, or sugar listed as the main ingredient. They have little to no (zero) fat or protein. Your body can absorb these items faster. This helps to bring your blood sugar up quickly.
Choose one of these rapid-acting sugars in these amounts:
- Chew 4 large glucose tabs. You can buy these at your local pharmacy without a prescription.
- Drink 4 ounces of fruit juice or soda (not diet soda).
- Chew 5 to 6 gummy candies or hard candies, such as LifeSavers®.
- Have 1 tablespoon of honey or syrup (not sugar-free syrup).
Do not eat chocolate, cookies, or a regular meal or snack to treat low blood glucose. Your body does not absorb these items very quickly. They may make your blood glucose even lower at first, then too high 1 to 2 hours later.
- Wait 15 minutes, then re-test your blood sugar. Re-test your blood sugar after 15 minutes. If your blood glucose is still less than 70 mg/dL, have another 15 grams of sugar. Re-test again 15 minutes later. Keep doing this until your blood glucose level is 70 mg/dL or higher.
Once your blood sugar is 70 mg/dL or higher, have your next meal or small snack within 1 hour. For example, a small snack may include one of the following:
- Peanut butter or cheese with 4 to 5 crackers.
- Half of a sandwich and 4 ounces of milk.
- A single-serve container of Greek yogurt.
What is severe hypoglycemia?
Hypoglycemia can get worse if you do not treat it quickly. Severe hypoglycemia happens when your blood glucose level goes below 54 mg/dL, or when you cannot take care of yourself.
Symptoms of severe hypoglycemia can include:
- Feeling very confused.
- Having trouble following directions or doing simple, routine tasks.
- Trouble speaking or slurred speech.
- Blurry vision or seeing double.
- Loss of balance or trouble walking.
- Suddenly feeling very weak or sleepy.
Talk with your family and friends about the signs of low blood sugar. Teach them what to do if you feel faint or become confused. If you become unconscious (pass out), someone must call 911 for an ambulance.
How to treat severe hypoglycemia
If your blood sugar is below 54 mg/dL, have 24 grams of simple, rapid-acting sugar instead of 15 grams. Choose one of these:
- Chew 6 large glucose tabs. You can buy these at your local pharmacy without a prescription.
- Drink 6 ounces of fruit juice or soda (not diet soda).
- Chew 8 to 9 gummy candies or hard candies, such as LifeSavers®.
- Take 1 ½ tablespoons of honey or syrup (not sugar-free syrup).
Wait 15 minutes, then re-test your blood glucose. Keep doing this until your blood glucose level is 70 mg/dL or higher.
Once your blood sugar is 70 mg/dL or higher, have your next meal or small snack within 1 hour. For example, you can choose to eat one of the following:
- Peanut butter or cheese with 4 to 5 crackers.
- Half of a sandwich and 4 ounces of milk.
- A single-serve container of Greek yogurt.
Emergency glucagon treatments
An emergency glucagon treatment is a prescription medication used to treat severe hypoglycemia. Your healthcare provider may prescribe this if you are at a very high risk for severe hypoglycemia.
If your healthcare provider prescribed an emergency glucagon treatment, read About Emergency Glucagon Treatments for more information.
How to prevent hypoglycemia
It is always best to prevent hypoglycemia before it happens. You can usually do this by balancing your medications, what you eat, and your level of activity. Keeping this balance isn’t always easy. Your provider, diabetes educator, and dietitian can work with you to lower your risk of hypoglycemia.
Follow these steps to lower your risk of hypoglycemia:
- Check your blood sugar more often, especially if you have had hypoglycemia before.
- If you take diabetes medications, be sure to eat enough. Do not skip meals.
-
Talk with your provider before:
- Changing your medications.
- Starting a new exercise routine. Exercise causes your body to use extra glucose.
- Changing how much you eat.
- If you drink alcohol, talk with your healthcare provider about how to do so safely.
When to call your healthcare provider
Call your healthcare provider any time you have hypoglycemia. They may need to change your medication.
About Insulin for Diabetes and Treatment-Related Hyperglycemia
This resource explains what insulin is, how it works, and different types of insulin. It also explains what type 1 and type 2 diabetes are and how to manage them. It answers common questions about insulin and diabetes.
About insulin
Insulin is a hormone that lets glucose (sugar) go from your bloodstream into your cells. Your pancreas makes insulin and releases it into your bloodstream.
Your cells need glucose for energy. If your body does not have enough insulin, glucose stays in your bloodstream. This causes hyperglycemia (high blood sugar).
Hyperglycemia can make you feel tired or sick. It can also make it harder for your body to fight off infection. Read About Hyperglycemia (High Blood Sugar) to learn more.
About type 1 and type 2 diabetes
Type 1 diabetes mellitus (T1DM) is when your pancreas does not make insulin at all.
Type 2 diabetes mellitus (T2DM) is when your pancreas does not make enough insulin. Your pancreas may make less insulin over time. You may also have insulin resistance. This means your cells do not respond to the insulin your body makes. This causes glucose to stay in your bloodstream instead of entering your cells.
How to manage type 1 and type 2 diabetes
People with T1DM must always take exogenous (ex-AH-jin-us) insulin. Exogenous insulin is medicine you inject (take as a shot). It acts like insulin and replaces the insulin your body cannot make.
People with T2DM may need oral medicine (medicine you swallow) to help manage blood glucose levels. As your pancreas makes less insulin over time, you may also need exogenous insulin.
Some diabetes medicines make your pancreas release more insulin. But these medicines will not work if your pancreas cannot make any more insulin. If so, you’ll need to use exogenous insulin to control your blood glucose levels. Talk with your diabetes healthcare provider about how to manage your blood glucose.
When to take insulin
It’s important to take insulin at the right time. Your diabetes healthcare provider will tell you how much to take and when to take it. Taking doses of insulin and other diabetes medicine too close together can raise your risk for hypoglycemia (low blood sugar). Read About Hypoglycemia (Low Blood Sugar) to learn more.
It helps to make a routine for taking insulin. If you miss a dose of insulin, wait until your next scheduled dose. Do not take a dose to make up for a missed dose unless your diabetes healthcare provider tells you to.
What to discuss with your diabetes healthcare provider
Share important health information with your diabetes healthcare provider.
- Had an allergic reaction to diabetes medicines in the past.
- Have liver or kidney problems.
- Have blurry vision or vision changes that make it hard to see clearly.
- Have a severe (very bad) infection.
- Are being treated for heart failure or recently had a heart attack.
- Have problems with your circulation (blood flow). This includes neuropathy (tingling or losing feeling in your fingers and toes).
- Have trouble breathing.
- Drink alcohol.
Types of insulin
Rapid-acting insulin
Rapid-acting insulin starts working within about 15 minutes to lower your blood glucose. It can be used to lower your blood glucose during meals. It can also be used to treat high blood glucose when you’re not eating.
A dose of rapid-acting insulin lasts for about 4 hours.
Examples of rapid-acting insulin include:
- Aspart (Novolog®, Fiasp®)
- Lispro (Humalog®, Lyumjev™)
- Glulisine (Apidra®)
Taking insulin doses too close together can cause hypoglycemia. Take doses of rapid-acting insulin at least 4 hours apart. If your diabetes healthcare provider gives you different instructions, follow their directions.
Mealtime insulin dose
When you eat, your blood glucose rises fast. Rapid-acting insulin is often called a mealtime insulin dose because it manages your blood glucose during meals. If you wait too long to eat after taking your mealtime insulin dose, this can cause hypoglycemia.
Take your mealtime insulin dose no more than 15 minutes before a meal. It’s best to wait until your meal is in front of you and you’re ready to eat. This helps prevent hypoglycemia.
Correctional insulin dose
A correctional insulin dose is when rapid-acting insulin is used to treat high blood glucose levels when you’re not eating. This dose is usually lower than a mealtime insulin dose.
Short-acting insulin
Short-acting insulin can take up to 1 hour to start working and lasts for 6 to 8 hours. If you’re taking it before a meal, take it 30 minutes before you eat. This gives the insulin enough time to start working.
Examples of short-acting insulin include regular human insulin (Humulin R and Novolin® R).
Intermediate-acting insulin
Intermediate-acting insulin usually takes about 2 hours to start working. It lasts for about 12 hours. Intermediate-acting insulin is often used to manage steroid-induced hyperglycemia. This is hyperglycemia caused by steroids, such as prednisone or dexamethasone.
If you’re taking intermediate-acting insulin for steroid-induced hyperglycemia, take the insulin and the steroid together. Do not take the insulin without taking the steroid unless your diabetes healthcare provider tells you to.
Tell your diabetes healthcare provider if your steroid dose changes, is held, or stopped suddenly. They may need to stop or adjust your insulin dose.
Examples of intermediate-acting insulin include Neutral Protamine Hagedorn insulin (Humulin N and Novolin® N). Neutral Protamine Hagedorn is also called NPH.
Long-acting insulin
Long-acting insulin is also called basal insulin or background insulin. Long-acting insulin works slowly over a long period of time. It works to keep glucose levels stable when you’re not eating, such as between meals or while you sleep. Long-acting insulin is not used to control the quick rise in glucose caused by eating.
Long-acting insulin starts working in about 2 hours. Some insulin lasts 20 to 24 hours. These include glargine (Lantus®, Basaglar®, Semglee®, and Rezvoglar™). Other insulin, such as insulin glargine U-300 (Toujeo®) and insulin degludec (Tresiba®), lasts 36 to 42 hours.
Take long-acting insulin at the same time every day unless your diabetes healthcare provider gives you other instructions. It’s helpful to set an alarm or reminder on your smartphone.
Common questions about diabetes and insulin
Will I become addicted to or dependent on exogenous insulin?
No. Taking exogenous insulin injections (shots) does not cause your body to make less insulin. If your body makes insulin, it will keep making it just the way it did before.
You can use exogenous insulin for short periods of time, such as during treatment.
Certain medicines cause hyperglycemia, but only while you’re taking them. These include steroids and some chemotherapies. Once you finish the treatment with these medicines, your blood glucose goes back to what it was before.
Tell your diabetes healthcare provider if your dosage of steroids or chemotherapy changes. You may need to change how much insulin you take, too. Follow your diabetes healthcare provider’s instructions.
What are the side effects of exogenous insulin?
Exogenous insulin is very similar to the insulin your body makes. This means it does not have many side effects.
The most common side effect of exogenous insulin is hypoglycemia. You can prevent this by taking your insulin as prescribed, knowing your blood glucose levels, and not skipping meals.
Tell your healthcare provider if you develop a rash. This is rare but may be a sign of an allergy.
Why can’t I just take a pill?
Oral diabetes medicine will only help your body do the things it usually does better. It cannot make your body do something it cannot already do. For example, if your pancreas cannot make more insulin, you may need to take insulin injections. Read About Oral and Non-Insulin Injectable Diabetes Medicine to learn more.
Can taking exogenous insulin cause problems with my eyesight? Can it affect how well my kidneys work? Can it make me lose my fingers, toes, or legs?
Some people do not want to start insulin until they can no longer delay taking it. But waiting too long can cause other health problems. Uncontrolled high blood glucose over long periods of time can cause eyesight loss. It can affect how well your kidneys work. You may lose your fingers, toes, and legs.
It’s best to manage your blood glucose right away, before other health problems start.
You may have vision changes as insulin brings your blood glucose under control. Tell your healthcare provider if this happens.
Is it my fault that I need to take insulin? Did I not take good enough care of myself?
Your genetics are one of the main causes of diabetes. Over time, diabetes lowers your body’s ability to make enough insulin. This is mostly out of your control. It is not your fault that your body loses cells that make insulin. Eating too much sugar does not cause you to have diabetes.
About Oral and Non-Insulin Injectable Diabetes Medicine
This resource explains what oral and non-insulin injectable diabetes medicines are and how they help prevent hyperglycemia (HY-per-gly-SEE-mee-uh). Hyperglycemia is also known as high blood glucose (sugar).
Oral medicine is medicine you swallow. Non-insulin injectable diabetes medicine is diabetes medicine other than insulin that you inject. This resource also answers common questions about types of diabetes medicine.
About non-insulin diabetes medicine
Non-insulin diabetes medicine helps your body manage blood glucose. It helps your body prevent hyperglycemia better than it already does.
For example, some medicine helps your pancreas release more insulin than usual. Other medicine helps your body make less sugar than usual. This helps prevent hyperglycemia.
This type of medicine will not make your body do something it cannot already do. It can improve how your body does some things. For example, if your pancreas cannot make more insulin, you may need to take insulin injections.
- Have had an allergic reaction to diabetes medicines in the past.
- Have liver or kidney problems.
- Have a severe infection.
- Are being treated for heart failure or have recently had a heart attack.
- Have severe problems with your circulation (blood flow) or trouble breathing.
- Drink alcohol.
Knowing these things will help them make a plan to control your blood glucose safely.
Hypoglycemia
Hypoglycemia (HY-poh-gly-SEE-mee-uh) is also known as low blood glucose. It’s one of the major side effects of medicine that lowers blood glucose. Read About Hypoglycemia (Low Blood Sugar) to learn more.
Hyperglycemia
Hyperglycemia is also known as high blood glucose. This happens when too much glucose (sugar) builds up in your bloodstream. Read About Hyperglycemia (High Blood Sugar) to learn more.
Types of diabetes medicine
Oral diabetes medicine
Most diabetes pills should be taken with the first meal of the day. This is when they work best. Taking them with food can also help prevent upset stomach, nausea (feeling like you’re going to throw up), and hypoglycemia.
The risk of hypoglycemia is often higher if you take more than one diabetes medicine.
Try to eat regular meals. Avoid skipping meals if you can. Follow your diabetes healthcare provider’s instructions.
Swallow your diabetes pills whole with a glass of water. Do not chew them.
Some pills have a score line in the middle of the tablet you can break them into 2 parts. If it’s hard for you to swallow a whole pill, break it into 2 parts and take both parts.
Try to take your diabetes medicine at the same time every day. If you miss a dose of diabetes medicine, plan to take it at the next scheduled time. Do not take a double dose to make up for a missed dose. Talk with your diabetes healthcare provider to make a plan for what to do if you miss a dose.
Biguanides
Biguanides (bi-GWA-nidez) help your body use insulin better. They also lower the amount of sugar your liver releases into your bloodstream.
Biguanides have a lower risk for causing hypoglycemia. The risk for hypoglycemia is higher if you take them with other diabetes medicine.
Examples of biguanides include metformin (Glucophage®, Glucophage XR, Glumetza®, Fortamet®, and Riomet®). These can be used with most other diabetes medicine.
Upset stomach is the most common side effect when you first start taking metformin. This includes symptoms such as nausea, diarrhea (loose or watery poop), vomiting (throwing up), and gas. Tell your diabetes healthcare provider if you have an upset stomach. They may prescribe a lower dose so your body gets used to it, then slowly raise it over time.
If you’re having a test with intravenous (IV) contrast, you may need to stop taking metformin for 2 days after the test. Tell the doctor who ordered the test and the person doing the exam you’re taking metformin. Talk with your diabetes healthcare provider. They may give you another medicine to take during this time.
Sulfonylureas
Sulfonylureas (suhl-fuh-nuhl-YUR-ee-uhz) help your pancreas release more insulin into your bloodstream. They will only work if your pancreas can already make insulin.
Sulfonylureas have a moderate to high risk for causing hypoglycemia.
Examples of sulfonylureas include:
- Glipizide (Glucotrol®, Glucotrol XL)
- Glimepiride (Amaryl®)
- Glyburide (DiaBeta®, Glynase® PresTab®, Micronase®)
Tell your diabetes healthcare provider if you’re told to not eat or drink to prepare for a procedure or surgery. Also tell them if you’re sick or have nausea and vomiting that keeps you from eating or drinking. This can lower your blood glucose too much and raise your risk for hypoglycemia. They may tell you to stop taking sulfonylureas.
SGLT2 Inhibitors
SGLT2 inhibitors help control your blood glucose. They let your body get rid of more sugar when you urinate (pee).
SGLT2 inhibitors have a lower risk for causing hypoglycemia. The risk for hypoglycemia rises if you take them with other diabetes medicine.
Examples include:
- Canagliflozin (Invokana®)
- Empagliflozin (Jardiance®)
- Dapagliflozin (Farxiga®)
- Ertugliflozin (Steglatro®)
- Bexagliflozin (Brenzavvy®)
SGLT2 inhibitors can cause urinary tract infection (UTI) and yeast infection. Practice good personal hygiene to lower your risk of getting UTI and yeast infections. This includes keeping your genital area clean and dry. You should also wear cotton undergarments that fit properly and are not too tight.
SGLT2 inhibitors can cause dehydration and low blood pressure. Drink lots of fluids to prevent dehydration while taking SGLT2 inhibitors.
Tell your diabetes healthcare provider if you’re told to not eat or drink to get ready for a procedure or surgery. They may tell you to stop taking SGLT2 inhibitors a few days before.
Tell your diabetes healthcare provider right away and do not take your next dose of SGLT2 inhibitors if:
- You’re sick or have nausea and vomiting that keeps you from eating or drinking.
- Are dehydrated.
- Are sick such as with an infection or the flu.
- Have physical stress such as surgery.
These things can cause euglycemic diabetic ketoacidosis (DKA). Euglycemic DKA is when your body has DKA but your blood glucose is normal or near normal. This is a medical emergency that must be treated right away. Read Diabetic Ketoacidosis (DKA) and Ketone Urine Testing to learn more.
DPP-4 Inhibitors
DPP-4 inhibitors help your pancreas release more insulin into your bloodstream when needed, such as after you eat. They slow down digestion, which helps lower your appetite. They also lower the amount of sugar your liver makes.
DPP-4 inhibitors have a lower risk for causing hypoglycemia. The risk for hypoglycemia rises if you take them with other diabetes medicine.
Examples of DPP-4 inhibitors include:
- Sitagliptin (Januvia®)
- Saxagliptin (Onglyza™)
- Alogliptin (Nesina®)
- Linagliptin (Tradjenta®)
Side effects of DPP-4 inhibitors can include headaches, joint pain, and upper respiratory tract infection. DPP-4 inhibitors can also cause acute pancreatitis, but this is rare. This is when your pancreas gets irritated or inflamed over a short period of time.
Thiazolidinediones (TZDs)
Thiazolidinediones (tie-uh-ZOW-luh-deen-dai-ownz) lower insulin resistance. This means they help your cells better use the insulin your pancreas makes. They also make your liver release less sugar into your bloodstream.
TZDs have a lower risk for causing hypoglycemia. The risk for hypoglycemia rises if you take them with other diabetes medicine.
Examples of TZDs include pioglitazone (Actos®) and rosiglitazone (Avandia®).
TZDs work slowly when you first take them. It can take up to 2 to 3 months for them to work fully. It is safe to take TZDs with or without food.
A side effect of TZDs can include fluid retention. This is when your body holds on to extra fluid, causing swelling. Fluid retention can raise your risk for cardiovascular disease (CVD), such as congestive heart failure (CHF).
Meglitinides
Meglitinides (muh-GLI-tuh-nidez) help your pancreas release more insulin into your bloodstream.
Meglitinides have a moderate to high risk for causing hypoglycemia.
Examples of meglitinides include repaglinide (Prandin®) and nateglinide (Starlix®).
This medicine works very fast. Take it 15 minutes before you eat. Waiting too long to eat after you take the medicine raises the risk of hypoglycemia.
Side effects of meglitinides can include headaches and mild cold-like symptoms.
Non-insulin injectable diabetes medicine
GLP-1 agonists and Dual GIP agonists
GLP-1 agonists help your pancreas release more insulin into your bloodstream when needed, such as after you eat. They lower the amount of sugar your liver makes. They also make your stomach empty more slowly. This helps you feel less hungry, which may help you eat less.
GLP-1 agonists have a lower risk for causing hypoglycemia. The risk for hypoglycemia rises if you take them with other diabetes medicine.
Examples of GLP-1 agonists include:
- Dulaglutide (Trulicity®)
- Exenatide ER (Bydureon)
- Semaglutide (Ozempic®)
- Liraglutide (Victoza®)
- Lixisenatide (Adlyxin™)
- Exenatide (Byetta™)
Side effects of these medicines can include nausea, vomiting, and diarrhea. GLP-1 agonists can also cause acute pancreatitis, but this is rare. This is when your pancreas gets irritated or inflamed over a short period of time.
If you’re taking GLP-1 agonists, tell your surgery team before you schedule a surgery or procedure with anesthesia. You may need to stop taking this medicine up to a week before getting anesthesia. This is because GLP-1 agonists can cause aspiration. This is when food or liquid goes into your airway instead of your esophagus (food pipe). Talk with your surgeon about steps to take before your surgery or procedure.
Tell your diabetes healthcare provider if you or a family member has ever had medullary thyroid cancer or multiple endocrine neoplasia (MEN). If so, they may prescribe a different medicine.
How to Improve Your Blood Sugar With Your Diet
This information explains how to manage your blood glucose with your diet. It also explains how to manage cancer treatment side effects and your blood glucose at the same time.
About blood glucose and your diet
Glucose is a simple sugar. It is the main source of energy for cells and comes from the foods you eat. Many things can affect your blood glucose, such as:
- Stress.
- Medicine.
- Changes to your diet.
- Physical activity and exercise.
Some cancer treatments and their side effects can also make your blood glucose levels go up or down. Managing your blood glucose is an important part of your cancer care, and we’re here to help.
A big part of managing your blood glucose is understanding what to eat. This can feel overwhelming. A clinical dietitian nutritionist or diabetes educator can help you to create a plan that is best for you. They will base their recommendations on your health and health goals. If you’d like to talk with a clinical dietitian nutritionist or diabetes educator, ask your healthcare provider.
The best diet is personal and different for every person. Your ideal diet is based on your health, cancer treatment plan, blood glucose goals, and personal preferences. It’s also important to try to follow a well-balanced diet that gives you the nutrients your body needs.
About carbohydrates
There are 3 main types of nutrients:
- Carbohydrates, also called carbs.
- Fats.
- Proteins.
These main nutrients are sometimes called macronutrients or macros. Many foods have all three of these nutrients. Each of these nutrients can turn into glucose, but this process is much easier and faster with carbohydrates. This is why your body uses carbohydrates as its main source of energy.
The following table has examples of foods and drinks with carbohydrates and foods without carbohydrates.
| Foods with carbohydrates | Foods without carbohydrates |
|
|
How carbohydrates affect your blood glucose
It’s important to include carbohydrates in your diet. Your body breaks down carbohydrates into glucose. Glucose is then released into the bloodstream where your cells can use it for energy.
While carbohydrates give your body energy, they also affect your blood glucose levels. Not all carbohydrates raise your blood glucose the same way. Some raise your blood glucose levels very quickly, while others raise them more slowly (see Figure 1). This can make it hard to manage your blood glucose.

Eating too many carbohydrates can increase your risk of high blood sugar (hyperglycemia). It’s important to keep your blood glucose from getting too high or too low (hypoglycemia).
The amount of carbohydrates you need is different for each person. For example, if you have type 1 diabetes mellitus (T1DM), you must have carbohydrates in your diet. Your healthcare provider will work with you to figure out your blood glucose goals and carbohydrate needs.
Your healthcare provider or diabetes educator will set your blood glucose target numbers. Keeping your blood glucose near those target numbers is an important part of your treatment.
About dietary fiber
Fiber is a type of carbohydrate. It slows down how quickly your body absorbs sugar. This helps manage your blood glucose levels.
There are two different types of fiber:
- Soluble fiber breaks down in water to form a gel. It is easier for your body to digest. Soluble fiber helps control blood glucose levels by slowing down how fast your body uses carbohydrates.
- Insoluble fiber does not dissolve in water. Because of this, it can help move stool (poop) through your body.
Tips to help you manage your blood glucose with your diet
Manage your blood glucose with carbohydrates
Here are some ways to manage the amount of carbohydrates you have in your diet.
Plate method
To help control carbohydrate portions, it can be helpful to follow the plate method. To do this:
- Fill ½ your plate with non-starchy vegetables, such as spinach, broccoli, or peppers.
- Fill ¼ of your plate with lean proteins, such as chicken, turkey, or seafood, including shellfish.
- Fill ¼ of your plate with high fiber carbohydrates, such as brown rice, sweet potatoes, or quinoa.
Limit the amount of carbohydrates in your meals, when needed
If your blood glucose is high, having meals with fewer carbohydrates can help bring it back to your target range. Never stop eating all carbohydrates, especially if you take insulin. This can make your blood glucose go too low. Talk with your healthcare provider for more information.
Here are some ways to have less carbohydrates in your meals:
- Have 1 main source of carbohydrate in your meal instead of 2. For example, have either whole grain rice or beans instead of both.
- Have an open-faced sandwich on one slice of bread instead of two.
- Drink sugar-free, flavored water and sparkling water instead of fruit juice or soda. Fruit juice made with real fruit usually has a lot of sugar.
- Substitute or add more protein, such as an egg, to your breakfast instead of having more bread or fruit.
- Limit refined grains, such as boxed pastas or some cereals.
- Choose whole foods instead of processed foods when you can. For example, choose apples instead of applesauce.
For people taking diabetes medicine
If you take diabetes medicine, talk with your healthcare provider or diabetes educator before lowering the amount of carbohydrates you eat and drink. If you lower the amount of carbohydrates you eat by too much, you could be at risk for low blood glucose (hypoglycemia). To learn more, read About Hypoglycemia (Low Blood Sugar).
Counting carbohydrates to manage your blood glucose
Carbohydrate counting is when you plan and track meals that have a certain number of grams of carbohydrates per meal. Carbohydrate counting helps you manage your blood glucose levels with the food you eat. This type of meal plan is often recommended for people taking insulin.
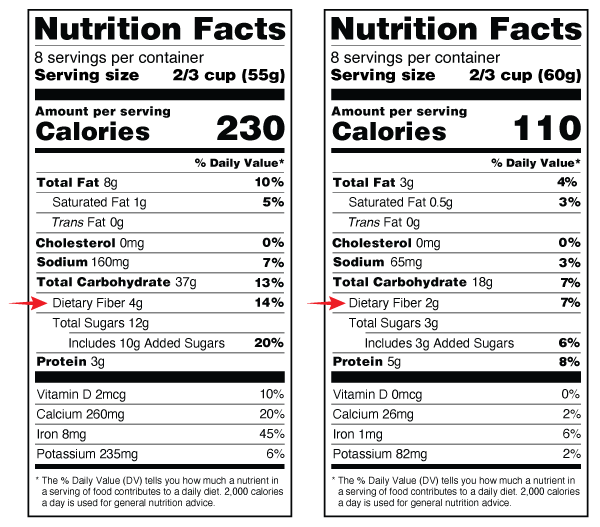
When you’re counting carbohydrates, use the number in the “Total Carbohydrate” row in the Nutrition Facts label (see Figure 2). Aim for 45 to 60 grams total carbohydrate at each meal. If your endocrinologist or diabetes educator recommends a different amount, follow their instructions. See the “Sample menus” section at the end of this resource for ideas for meals that meet these carbohydrate goals.

During your treatment, your doctor may ask you to track or change the amount of carbohydrates in your diet. This is to help manage your blood glucose levels. Always talk with your clinical dietitian nutritionist, diabetes educator, or doctor before changing the amount of carbohydrates in your diet.
Difference between grams listed on Nutrition Facts labels
Sometimes both the serving size and the amount of carbohydrates in a serving can be measured in grams. But they are not the same.
- Grams (g) listed next to the “Serving Size” tells you the weight of the food item in grams. If you are using a food scale, you can use this information to measure the serving size (see Figure 3).
- Grams (g) listed next to “Total Carbohydrate” tells you the amount of carbohydrate in one serving of the food (see Figure 3).

Steps to carbohydrate counting
Step 1: Talk with your care team to decide the amount of carbohydrates you should have at each meal.
Step 2: Include foods in your meal that have carbohydrates. Use examples in the “About carbohydrates” section of this resource. Talk with a clinical dietitian nutritionist or diabetes educator to learn more.
Step 3: Calculate the grams of carbohydrates (per serving) for the food you’re eating. To do this, use the Nutrition Facts label to find the serving size and total grams of carbohydrates per serving (see Figure 3).
Step 4: Calculate the total amount of carbohydrates by adding the grams from each source of carbohydrate. For example, a serving of Cheerios and 1 cup of 1% milk has 41 grams of carbohydrates (see Figure 4).

Carbohydrates in 1 serving size (1 ½ cups or 32 g) of Cheerios = 29 g
Carbohydrates in 1 serving size (1 cup) of 1% low fat milk = 12 g
Total carbohydrates (29 g + 12 g) = 41 g
Step 5: Measure your foods to the serving size on the food label (see Figure 4). You can use a measuring cup or a kitchen scale. It’s important to measure your food initially so that you get used to what the serving size is. But after you become used to what the serving size looks like, it’s OK to estimate your measurements. They don’t need to be exact. Talk with your clinical dietitian nutritionist for more information about measuring your serving sizes.
What to do if you do not have a Nutrition Facts label
If a food does not have a Nutrition Facts label or you’re eating out, search for the carbohydrate information online. Some websites, such as www.CalorieKing.com and www.MyFitnessPal.com, also have mobile applications (apps) for your smartphone or tablet. Talk with a clinical dietitian nutritionist for more resources.
For people taking insulin
If you’re taking insulin, your healthcare provider can show you how to measure your insulin dose for each meal. Talk with your healthcare provider or diabetes educator for more information.
How to manage your blood glucose with fiber
Another way to manage your blood glucose is to choose carbohydrates that have more fiber and less sugar. Choose foods with more than 3 grams (g) of fiber per serving. These include foods such as foods such as oats, peas, beans, apples, citrus foods, and barley.
It’s important to eat high-fiber foods that have soluble fiber, such as:
- ¾ cup to 1 cup serving of multi-grain cereal.
- ½ cup of cooked beans or lentils.
- 3 cups of air popped popcorn.
- 1 medium potato or sweet potato.
It can be hard to only eat carbohydrates that are high in fiber. Try to switch out low-fiber foods with high-fiber foods as often as you can.
You can find the amount of fiber in packaged foods by reading the Nutrition Facts label. The Nutrition Facts label has information about the amount of certain nutrients in the food or drink. The amount of fiber is listed in the “Dietary Fiber” row (see Figure 5).
How to manage nutrition during cancer treatment
During cancer treatment, side effects can limit your ability to eat well. Side effects can include nausea (feeling like you’re going to throw up), taste changes, or appetite loss (not wanting to eat).
Being unable to eat can raise your risk for weight loss. It also raises your risk for malnutrition (when your body does not get all the nutrients it needs).
Read Eating Well During Your Cancer Treatment to learn more about general nutrition guidelines during cancer care.
If you’re having a hard time eating during treatment, talk with your healthcare providers and clinical dietitian nutritionist. You may need to change your diet to get the nutrients you need. Sometimes, they may want you to focus less on carbohydrate counting.
Eating small meals more often can make it easier to meet your nutrition goals. Your clinical dietitian nutritionist can help set your carbohydrate goals for each smaller meal. Focus on eating more protein and healthy fats. This will help you get the nutrients you need as you manage your blood glucose.
Here are some examples of foods with proteins and healthy fats:
- Nuts and nut butters.
- Seeds, such as pumpkin seeds or flax seeds.
- Avocados.
- Unsweetened (plain) yogurt and cheese.
- Lean protein, such as fish, chicken, eggs, and tofu.
- Olive oil and canola oil.
Diet changes can help. But you still may need medicine to manage side effects better. If you’re prescribed medicine, be sure to follow your care team’s instructions for taking them.
How to manage loss of appetite during cancer treatment
Appetite loss means you have less of a desire to eat. It’s a very common side effect of treatment. When you lose your appetite, you may want to eat comfort foods to feel better. This can make it harder to eat a well-balanced diet and manage your blood glucose levels.
Try these tips to help you get the most from your meals when you can’t eat much:
- Add more protein to your diet, such as chicken, fish, eggs, or tofu.
- Have a protein shake or nutritional supplement that’s high in protein and low in carbohydrates. Some are high-calorie, ready-made drinks that have vitamins and minerals added to them. Others are powders that you can mix into other foods or drinks. Most are also lactose-free. That means you can have them even if you’re lactose intolerant (have trouble digesting milk products). Talk with a clinical dietitian nutritionist for suggestions.
- Talk with your healthcare provider about your symptoms. They may give you a prescription for a medicine to help with your appetite.
It’s hard to manage your blood glucose while going through cancer treatment. Sometimes you need more than the right diet and exercise routine. If you’re having trouble managing your blood glucose, talk with your care team.
Sample menus
Your care team may tell you to aim for 45 to 60 grams of carbohydrates per meal. Follow your care team’s instructions. Do not eat more than 60 grams of carbohydrates at any meal.
Aim to have about the same mount of carbohydrates at each meal:
- 3 to 4 servings (45 to 60 grams) of carbohydrates for breakfast.
- 3 to 4 servings (45 to 60 grams) of carbohydrates for lunch.
- 3 to 4 servings (45 to 60 grams) of carbohydrates for dinner.
Below are sample menus with ideas for meals and snacks that meet these carbohydrate goals. These menus are meant to be examples. Each menu shows how many grams of carbohydrates are in each item.
| Meal Time | Sample menu 1 | Sample menu 2 |
Breakfast (based on 45 to 60 g carbohydrates)
| 1 small orange (15 g) ½ avocado (10 g) 2 scrambled eggs (0 g) 1 whole wheat English muffin (22 g) 1 teaspoon butter (0 g) 1 cup coffee (0 g) | 2 cups Cheerios (40 g) 1 cup 1% milk (12 g) 1 tablespoon peanut butter (0 g) 1 cup coffee (0 g) |
| Lunch (based on 45 to 60 g carbohydrates) | 4-ounce hamburger (0 g) 1 slice of American cheese (0 g) 1 slice lettuce, tomato (1 g) 1 hamburger bun (22 g) 1 small apple (15 g) 1 ounce salted hard pretzels (22 g) 1 cup water (0 g) | 4 oz. turkey (0 g) 1 slice lettuce, tomato (1 g) 2 slices rye bread (32 g) 1 ounce snack pack of baked Lays chips (24 g) 12 ounces seltzer with lime slice (0 g) |
| Dinner (based on 45 to 60 g carbohydrates) | 4 ounces baked chicken with breading (10 g) 1 white cup rice (44 g) 2 cups broccoli (0 g) 12 ounces seltzer (0 g) | 2 ounces cooked ziti pasta (44 g) ½ cup tomato basil sauce (10 g) 2 cups tossed salad (0 g) 1 cup mixed raw salad veggies (0 g) 1 tablespoon oil (0 g) 1 tablespoon vinegar (0 g) |
Follow-up care
Within 1 week after discharge
It’s important to share your blood glucose readings with your outpatient diabetes healthcare provider within 7 days after you’re discharged. You may need to talk to them sooner if:
- You were just diagnosed with diabetes or hyperglycemia.
- You were discharged with a feeding tube.
- You’re tapering off steroids.
- You’re trying to get your blood glucose to a target range to continue treatment.
- Your medicine regimen (the medicines you take) has changed.
- Your blood glucose levels are not within your target range.
Some of your healthcare providers often do not manage blood glucose levels or adjust diabetes medicine. This can include your oncologist (cancer doctor), surgery team, or radiation oncologist.
Follow up with your primary healthcare provider or diabetes healthcare provider to manage your blood glucose levels after you’re discharged. If you do not have a primary healthcare provider or endocrinologist, tell a member of your care team. They can help set up follow-up care.
Routine follow-up
Certain appointments and testing are recommended as routine care for people with diabetes. It’s how we check for problems caused by diabetes early, when they’re easier to treat.
You can use the logs at the end of this resource to help keep you on track during your care.
Educational resources
This section lists the MSK educational resources mentioned in this guide. Always read the written version even if you watch the video. There’s important information in the written version that may not be in the video.
- Contour® Next One Video: Doing Your First Test
- www.contournextone.com/getting-started
- How to Store and Get Rid of Your Home Medical Sharps
- Diabetic Ketoacidosis (DKA) and Ketone Urine Testing
- How To Check Your Blood Glucose (Blood Sugar) Using a Blood Glucose Meter
- About Your Continuous Glucose Monitor (CGM)
- About Emergency Glucagon Treatments
- Managing Nausea and Vomiting
- Managing Taste Changes During Chemotherapy
- www.CalorieKing.com
- www.MyFitnessPal.com
- Using Your Insulin Pump or Continuous Glucose Monitor (CGM) Safely While You’re at MSK
More diabetes resources
American Diabetes Association (ADA)
www.diabetes.org
The ADA has helpful tips for diabetes self-care, diet, and recipes with nutrition information.
Joslin Diabetes Center
www.joslin.org/diabetes-information
